Sexual and reproductive health and rights in Sweden 2017
Summary
New knowledge about SRHR in Sweden
Experience of sexual harassment and assault is common among women
Sexual harassment, assault, and sexual violence constitute serious threats against peoples’ safety and health. Research has shown how common sexual violence is and has identified the many different negative health consequences it brings. Sexual violence affects peoples’ physical, sexual, reproductive, and mental health negatively.
SRHR2017 shows that many different forms of sexual harassment and sexual assaults are common in the population. Women are more often victimized than men, and LGBT persons are more often victimized than the general population. Younger individuals are also more often exposed than older individuals.
Almost half of women (42 percent) in Sweden have been subjected to sexual harassment, as have 9 percent of Swedish men. The proportion among women aged 16–29 is more than half (57 percent). More than every third woman (39 percent) and almost every tenth man (9 percent) have been subjected to some form of sexual assault. As with sexual harassment, more than half of women aged 16–29 (55 percent) have been the victim of some form of sexual assault.
Eleven percent of women and one percent of men have been victims of attempted rape through physical violence or threat of violence. LGBT people have experienced this to a higher degree than heterosexuals, and about 30 percent of lesbians and 10 percent of gay men have experienced this.
There are differences related to level of educational attainment. Women with lower education are more often subjected to sexual harassment and to sexual assault compared to women with higher education. These distinctions are probably due to differences in knowledge about and awareness of the meaning of sexual harassment.
Women with lower educational level are also more often the victims of rape enforced by physical violence or threat of violence compared to women with higher educational level.
The majority are satisfied with their sex life, but there are large differences between the genders
Human sexuality is an important part of life and has a significant effect on health. Our sexuality is linked to our identity, integrity, and intimacy. These in turn affect, among other things, our self-esteem, our well-being, and our resiliency. Measuring experiences of peoples’ sex lives and sexual habits is not without its difficulties. Earlier studies have focused on how often people have sex, sexual transmitted infections, and sexual risk taking. The current study has a broader focus on SRHR and examined, among other things, sexual satisfaction and sexual dysfunctions.
The results show that the majority of the Swedish population is satisfied with their sex life, find sex important, and have had sex during the past year. The youngest men (aged 16–29) and the oldest men and women (aged 65–84) were the least satisfied.
Sexual experiences and sexual dysfunctions differed depending on gender. It was more common among men to be without a sex partner compared to women. It was also more common among men to have had premature orgasms, to not have had sex the way they wanted to, and to want more sex partners. Seventeen percent of men reported erectile dysfunctions. On the other hand, women more often reported lack of interest in sex, low sex drive, lack of feelings of pleasure, lack of sexual arousal, pain during or after sex, and lack of orgasms.
Considerably more women reported to have been too tired or too stressed to have sex during the past year, especially in the age span of 30–44 years. Eight percent of the population reported health problems or physical problems that negatively affected their sex life, and 13 percent had sought health care for their sexual problems.
Another influencing factor is sexual identity and transgender experience. Regardless of sexual identity, the majority reported being satisfied with their sex life. However, both bisexual women and men reported more often that they were dissatisfied with their sex life compared to other groups. Most LGBT people and heterosexuals had had sex in the past year, although every fourth trans and every fifth bisexual man reported not to have had sex. A lower percentage of trans people were satisfied with their sex life, but trans people aged 45–84 were more satisfied than the younger age groups.
Women’s and men’s experiences of their sex life differ, and the differences are most pronounced during the reproductive years. Deeper analyses are needed to better understand these differences and to improve knowledge on what consequences these can have on relations, life in common, and people’s well-being. The need of support in relation to sexuality ought to be met by accessible and needs-oriented information, counselling, and care.
Women feel freer to take initiative and to say no to sex than men
Integrity, voluntariness, and sexual consent are prerequisites for good sexual health. Free decision making over one’s body is also a human right. The concept of sexual empowerment describes an individual’s perception of autonomy and decision making over when, how, and with whom to have sex.
The results show that a majority of the population think sex is important in a romantic relationship, feel free to take sexual initiative, can say no to sex, know how to suggest to a partner how they want to have sex, and know how to say no if a sex partner wants to do something they do not want to do. Approximately half of women and men reported that they and their partner equally often decide when and where to have sex. It was more common for men to report that their partner decided where and when to have sex. A larger percentage women, as compared to men, most often feel free to take sexual initiatives, know how to say no to having sex, know how to suggest how to have sex, and know how to say no if a sex partner want to do something they do not want to do.
Men with shorter education feel freer to say no to having sex compared to men with lower educational level. Women with university education are more likely to find sex to be important in relationships, know how to take the sexual initiative, and tend to more often be able to tell a partner how they want to have sex.
All sexual activity is to be voluntarily in Sweden, and it is a criminal offence to force someone to partake in sexual activities against their will. Sexual consent and voluntariness are prerequisites for good sexual health. It is important to spread information to young people, and schools are an important arena for this. Schools are a place where one early on can discuss ethics and basic human values and the right of all humans to make decision over their own bodies.
Most people know how to communicate if and how they want to have sex
Sexual communication and consent can be complicated to handle in practice because it is dependent on, for example, the context and the people involved. The ability to communicate in sexual situations might lead to different health outcomes. In the same government assignment, the study “Sexual communication, consent and health” was performed via the Novus Sverigepanel and included 12,000 participants.
The results show that most people reported that they have the ability to communicate if and how they want or do not want to have sex. Women, younger people, and those who live in a relationship reported this more often. The most common ways to communicate were verbally or with body language and eye contact. Sexual communication varied based on gender, education, and relationship status, among other things.
One third of the respondents think that their communication skills do not affect their wellbeing. One quarter feel that their communication skills make them feel better, and another quarter reported that these skills make them feel safer in sexual situations. One tenth feel insecure and stressed in sexual situations as a result of their communication skills.
Twice the number of women as men have complied with having sex
The Novus survey also shows that 63 percent of women and 34 percent of men have complied with having sex at least once even though they did not really want to. Reasons to comply were they did it for their partner's sake, for the relationship, or due to expectations. This was especially true for women. More women than men also ended ongoing sex. Bisexual women have more often complied with having sex even though they did not really want to compared to lesbians and heterosexual women. It was also more common among gay men and bisexual men to comply with having sex compared to heterosexual men.
Men stated to a greater extent that it has not been relevant to express that they do not want to have sex or that they do not want to have sex in a certain way, to comply with having sex, or to end ongoing sex.
The results therefore show that how one communicates what one wants and does not want to do when one has sex depends on gender, relationship status, educational attainment, age, sexual identity, and the situation itself. More knowledge is needed on how sexual communication is affected by masculinity and femininity norms together with other power structures such as heteronormativity.
Seventy percent of men consume pornography, while 70 percent of women do not
Pornography is widely debated, and research has found both negative and positive consequences of pornography consumption. Pornography is said to increase the acceptance of sexuality, sexual identities, and different sexual practices and to act as a source of inspiration. Research has also pointed out negative consequences of frequent pornography consumption on, for example, attitudes, behaviors, and sexual health. Frequent pornography consumption is, among other things, associated with more accepting attitudes toward violence against women, a tendency to want to try sexual activities inspired by pornography, and increased sexual risk taking. This is probably due to the content of pornography today, which to a large extent constitutes violence against women and male dominance. From a public health perspective, the aim of this survey was to explore how pornography consumption affects people’s sex life, sexual well-being, and general health.
The results show that many women and men of all ages use the Internet for sex-related activities such as looking for information, reading sexually arousing texts, or looking for a partner. Almost all activities are most common among younger people and decrease with age. There are few differences in Internet use for sex-related activities among young people. It is more common among older men to use the Internet for sexual activities than among women.
Pornography consumption is much more common among men than among women, and it is more common among younger people compared to older people. A total of 72 percent of men report that they consume pornography, while the opposite is true for women, and 68 percent never consume pornography.
Forty-one percent of men aged 16 to 29 are frequent users of pornography, i.e. they consume pornography on a daily basis or almost on a daily basis. The corresponding percent among women is 3 percent. Our results also show an association between frequent pornography consumption and poorer sexual health, and an association with transactional sex, too high expectations of one’s sexual performance, and dissatisfaction with one’s sex life. Almost half of the population state that their pornography consumption does not affect their sex life, while a third do not know if it affects it or not. A small percentage of both women and men say their pornography use has a negative effect on their sex life. It was more common among men with higher education to regularly use pornography compared to men with lower education.
There is a need for more knowledge on the link between pornography consumption and health. An important preventive piece is to discuss the negative consequences of pornography with boys and young men, and school is a natural place to do this. Education on gender equality, sexuality, and relationships are mandatory in schools in Sweden, and sexuality education is an important part of the preventive work for sexual health for all.
Almost 10 percent of men have paid for sex
Transactional sex is used to describe a situation where a person gets, or is offered, compensation or reimbursement in exchange for sex. The compensation can be money, clothes, gifts, alcohol, drugs, or a place to sleep. Since 1999 it is illegal to buy sex in Sweden, while selling sex is not.
To pay or in other ways reimburse someone in exchange for sex is mainly a male phenomenon. Almost 10 percent of men – but fewer than one percent of women – reported to have at least once paid for sexual favours. It was more common to have paid for sex abroad, and 80 percent of men who paid for sex did so abroad. No differences were found between men with different educational levels. Gay men and bisexual men had more often paid for sex compared to heterosexual men (nearly 15 percent and 10 percent, respectively).
One of the purposes when criminalizing the buying of sex was to change attitudes towards paying for sex. Changing these attitudes is part of the broader work for gender equality that has to be undertaken in every corner of society in order to reduce women’s vulnerability. To decrease the demand for prostitution is part of the overall goal to discontinue men’s violence against women.
The results also show that it is rare to accept payment in exchange for sex. Nevertheless, it is more common among LGBT people. It is also more common to accept payment in exchange for sexual favours in Sweden among both women and men than to do so abroad.
The reasons for accepting payment in exchange for sexual favours are diverse. Prevention should therefore include different actions from public authorities, the education sector, and the health care sector. Those concerned should be offered social support and social interventions that encourage good sexual, physical, and psychological health regardless of sex or sexual identity.
Reproductive health: results on contraceptives, pregnancy, abortion, miscarriage, children, and child delivery
Reproduction is a central part of life. Contraceptive use, thoughts about children, and reproductive experiences such as pregnancy, abortion, miscarriage, and child delivery are important parts of our reproductive health and are also closely linked to our psychological, sexual, and general health.
The results show that fewer women aged 16–29 use birth-control pills among those with higher income compared to women with lower income as well as among women with higher education compared to those with lower education. The differences in use are probably due to differences in knowledge and fear of hormones and their side effects.
A third of all women reported they have had at least one abortion. This proportion, as well as the percentage who have experienced a miscarriage, has remained unchanged since the 1970s.
When women reported about their child deliveries, 26 percent said they had entailed physical consequences, 17 percent reported psychological consequences, and 14 percent reported sexual consequences. These consequences differ depending on age and educational attainment. Partners participating during the delivery of their child were also affected psychologically, physically, and sexually, although to a lesser extent. The majority of women with experience of child delivery had had an episiotomy or a spontaneous laceration, while 4 percent had a rupture involving the anal sphincter (grade 3 or 4). Approximately one tenth had sought care for problems related to the episiotomy or spontaneous lacerations in relation to delivery. Neither age, education level, nor income affected the seeking or receiving of care or problems related to child delivery.
Most people reported that they have the number of children that they want, except for men with lower education. Three percent are involuntarily childless, whereas 5 percent in all age brackets do not want children. Approximately 7 percent of both women and men aged 30 to 84 have become parents without wanting to.
In conclusion, SRHR2017 showed that use of contraceptives among women in Sweden varies depending on age and need, but also on income and educational level. Reproductive experiences such as pregnancy, abortion, miscarriage, and child delivery vary depending on a range of factors such as age, income, education, sexual identity, and sometimes region. Further knowledge on associations with more variables is needed to know how to best go about addressing inequities in reproductive health.
SRHR – an issue of gender equality and equity
SRHR2017 showed differences in sexual and reproductive health and rights between different groups in the population. The answers to almost all questions in the survey differed between women and men, and the greatest gender differences were seen for:
- sexual harassment and sexual violence
- experiences of payment in exchange for sex
- pornography use
- several different experiences in people’s sex lives
This reflects different gender conditions regarding sexual and reproductive health. Further, the results show greater vulnerability among women, younger people, non-heterosexuals, and trans people and to a certain degree among people with lower income and education.
A majority of the population have good sexual health, which of course is a positive result. At the same time, sexuality and people’s sex lives differ, sometimes a lot, between women and men. For example, women more often experience low sex drive because of fatigue and stress compared to men. Why men less often feel free to say no to sex needs to be studied further. There are strong norms in our society regarding sex and sexuality, and gender roles, norms regarding femininity and masculinity, and norms regarding heterosexuality affect to what extent people feel free to live their lives as they see best.
Sexual harassment, assault, and sexual violence and how these affect our health is an important public health issue. The prevalence and the consequences do not just affect the victimized individual; they are also a marker for how equal a society is.
Based on the results of SRHR2017, there appears to be a need for more discussions and analyses on sexuality regarding support, advice, and education. For young people we have youth clinics and maternity health care centers where issues related to sex also can be discussed – but that mainly target women – and there are few places where older people can turn to receive help regarding their sex life and sexuality. There is a need to systematically monitor and evaluate these preventive institutions, especially youth clinics, also because of the need of men for support, advice, and care related to their sexuality. We need to emphasize the reproductive rights and health of men and discuss men’s rights to reproductive health, the path to having children, their use of contraceptives, treatment for sexually transmitted diseases, and general sexual health.
In SRHR2017, we see that women and men of all ages use digital arenas for sexual purposes. Young people are more active online, and differences between the sexes are small among young people. UMO.se is an online youth clinic and a good example of how to handle sexuality issues in way that reaches many and with high quality.
Schools are important arenas for improving gender equality and equity regarding health, and the sex education in schools constitutes an important part of SRHR. Sex education in schools and school health care are to provide information to all students about structural perspectives, like legislation and norms, and individual perspectives, such as the physical body, sexual health, relationships, and sexuality. Studies show that students receive more information on sexual health, pregnancy, and contraceptive use than about gender equality, LGBT perspectives, and relationships even though sex education has been subjected to improvements such as integration into other subjects. The improvement work with sex education is supported by a quality assessment from the School Inspection, improvements from the School Authority, and international guidelines regarding sex education from UNESCO and WHO Europe.
SRHR in Sweden – how to proceed
Sweden has a unique opportunity to reach gender-equal sexual and reproductive health and rights based on Swedish legislation, UN conventions, and established policy documents. Sweden has a strong political consensus, which is also reflected in Agenda 2030.
Sexuality is a determinant of health, and the interplay between structural, socioeconomic, demographic, and biological factors influences sexual health. Sexuality and sexual health are dependent on many other aspects of health and lifestyle factors, such as mental health and the use of alcohol and drugs.
In conclusion, our results confirm our prior understanding of SRHR, namely that social prerequisites are crucial for people’s freedom and sense of control over their sexuality and reproduction and to have good sexual, reproductive, mental, and general health. Gender differences exist due to structures, norms, and expectations on both the individual level and societal level, and this creates patterns that affect people’s sex life, communication, relationships, and family life in relation to health.
An important public health issue is sexual harassment, assault, and sexual violence and how this negatively affects health. Harassment, assault, and sexual violence have to stop.
We need further knowledge on differences due to gender, socioeconomic status, and sexual identity in order to improve gender equality and equity. The conditions for and the rights to sexual health need to be monitored and analyzed.
SRHR is coordinated on a national level by The Public Health Agency of Sweden, which works to improve knowledge and national cooperation. In the monitoring of the sustainable development goals, the Swedish gender equality policy, and the strategy to end men’s violence against women, the SRHR issues and specific items from this material are essential. The knowledge generated by this study is a starting point for further public health improvements within the field of SRHR in Sweden.
To examine sexual and reproductive health and rights
The Public Health Agency of Sweden coordinates SRHR nationally, builds knowledge, and monitors SRHR in Sweden. The purpose with the government’s assignment for the agency to perform a population survey on SRHR was to increase knowledge and by doing so create better conditions for SRHR in Sweden.
Paradigm shift in sexuality issues
The link between sexuality and health has been investigated previously. Sweden performed the first population-based sexuality survey in the world in 1967. After ten years of preparation, the former Public Health Institute of Sweden undertook, on assignment from the government, the study “Sex in Sweden” in 1996. This study is often cited concerning sexuality and health issues, largely due to the lack of larges studies on the topic.
During the past 20 plus years since 1996, several important changes and reforms have been passed. In the time line below, we show a selection of these societal changes. Some of the greatest changes are the introduction of the Internet, improved rights for LGBT people, and Sweden’s membership in the EU, which together with increased globalization have increased the mobility of people and services.
Figure 1. Time line with some of the changes in the SRHR field since 1996.
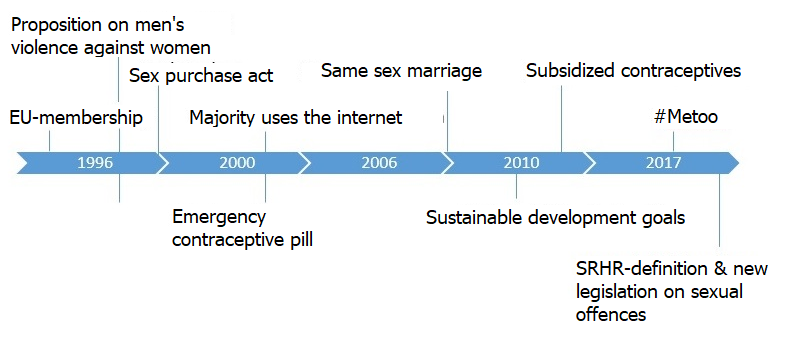
When the Public Health Agency in 2017 conducted the survey described here, it was done in a new context for SRHR. This is most evident regarding gender equality and feminism, norm awareness, improved LGBT rights, and of course the Internet. In addition, the Guttmacher–Lancet commission for sexual and reproductive health and rights developed a thorough and evidence-based agenda with priorities for SRHR in 2018. Their definition of SRHR is:
Sexual and reproductive health is a state of physical, emotional, mental and social well-being in relation to all aspects of sexuality and reproduction, not merely the absence of disease, dysfunction or infirmity. Therefore, a positive approach to sexuality and reproduction should recognize the part played by pleasurable sexual relationships, trust and communication in promoting self-esteem and overall well-being. All individuals have a right to make decisions governing their bodies and to access services that support that right.
Achieving sexual and reproductive health relies on realizing sexual and reproductive rights, which are based on the human rights of all individuals to:
- have their bodily integrity, privacy, and personal autonomy respected
- freely define their own sexuality, including sexual orientation and gender identity and expression
- decide whether and when to be sexually active
- choose their sexual partners
- have safe and pleasurable sexual experiences
- decide whether, when, and whom to marry
- decide whether, when, and by what means to have a child or children and how many children to have
- have access over their lifetimes to the information, resources, services, and support necessary to achieve all of the above free from discrimination, coercion, exploitation, and violence
To monitor SRHR
The global goals of Agenda 2030 focus on improved gender equality and equity and on strengthening people’s sexual and reproductive health and rights. Many of the goals in Agenda 2030 are related to SRHR, foremost goal number 3 about health and well-being for all ages and goal number 5 about gender equality and the empowerment of all women and girls.
Following the development of SRHR in Sweden is central to being able to fulfill the global goals. This is largely due to the great gender differences and the differences between age groups. The definition of SRHR summarizes the key reasons for why women, children, and young adults are the focus in order to reach the global goals. Several authorities and other operators continually work with these issues together with the health care sector, the social services, and the schools as central arenas.
| Global Sustainable Development Goals | Targets |
|---|---|
| 3. Good health and wellbeing | 3.1 Reduce maternal mortality |
| 3. Good health and wellbeing | 3.2 End all preventable deaths under age 5. |
| 3. Good health and wellbeing | 3.3 By 2030, end the epidemics of AIDS, tuberculosis, malaria, and neglected tropical diseases and combat hepatitis, water-borne diseases, and other communicable diseases. |
| 3. Good health and wellbeing | 3.7 By 2030, ensure universal access to sexual and reproductive health-care services – including family planning, information, and education – and the integration of reproductive health into national strategies and programs. |
| 5. Gender equality | 5.1 End all forms of discrimination against all women and girls everywhere. |
| 5. Gender equality | 5.2 Eliminate all forms of violence against all women and girls in the public and private spheres, including trafficking and sexual and other types of exploitation. |
| 5. Gender equality | 5.3 Eliminate all harmful practices, such as child, early, and forced marriage and female genital mutilation. |
| 5. Gender equality | 5.6 Ensure universal access to sexual and reproductive health and reproductive rights. |
| 10. Reduced inequalities | 10.3 Ensure equal opportunity and reduce inequalities of outcome, including by eliminating discrimination. |
Method
The population-based survey SRHR2017 was a survey among the Swedish general population that was carried out by the Public Health Agency in collaboration with Statistics Sweden and Enkätfabriken AB. The survey included questions on general and sexual health, sexuality and sexual experiences, sexuality and relations, the Internet, payment in exchange for sexual favours, sexual harassment, sexual violence, and reproductive health. Therefore, the scope of SRHR2017 was much broader compared to that of “Sex in Sweden” from 1996. The SRHR2017 study was approved by the ethical committee in Stockholm (Dnr: 2017/1011-31/5).
The survey was sent by mail to a representative stratified sample of 50,000 individuals with help from the Total Population register. The response rate was 31 percent. The dropout rate was higher among people with lower education and among those born outside of Sweden. The percentage of dropouts was slightly higher than in general surveys about health, but similar to other surveys about sexuality and health. We used calibration weights to adjust for non-response and to be able to draw inferences to the total population. Still, the results should be interpreted carefully. SRHR2017 is the first population-based study on SRHR in Sweden, and the results are presented by sex, age-group, educational level, sexual identity, and in some cases for trans people.
In addition, the Public Health Agency performed a web survey during the fall of 2018 about sexual communication, sexual consent, and health among approximately 12,000 respondents from the Novus Sverigepanel. This panel contains 44,000 individuals who are randomly selected for different surveys. According to Novus, their panel is representative of the Swedish population regarding sex, age, and region within the age-bracket 18–79. The panel surveys often reach a response rate of 55–60 percent, and our survey had a response rate of 60.2 percent. For further information, please see the report ”Sexuell kommunikation, samtycke och hälsa” by the Public Health Agency of Sweden.
The survey SRHR2017 – background and methods
The Public Health Agency has performed a population based national survey on sexual and reproductive health and rights (SRHR). This report summarizes the background to the area of SRHR and the methods of the survey.
The survey focused on sexual and reproductive health as a health determinant from a perspective of public health, equity and gender equality. The questions regarded general and sexual health, sexuality and sexual experiences, sexuality and sexual relationships, internet, sex for compensation, exposure to violence and reproductive health. The focus was broader than in previous Swedish studies on sex life. The questions regard important factors with associations to health in the population.
The survey SRHR2017 was performed in 2017 in collaboration with Statistics Sweden and Enkätfabriken AB. The survey was sent out to a randomized stratified sample of the total population registry of approximately 50 000 individuals. The response rate was 31 per cent. The non-response rate was biased, with a higher non-response rate among people with for example lower education. The reasons for the non-response rate was similar to other surveys and was dealt with via weighting in order for the responses to represent the population of Sweden as far as possible.
The survey is the first large randomized population study on SRHR in Sweden and the results can be presented by sex, age, socioeconomic status and sexual orientation. A limitation is the high non-response rate and another is the fact that some questions asked for life-time prevalence while other surveys may ask for experiences during for example the past year. The results does not provide a complete picture of the state of SRHR but rather provides new and updated knowledge.
Sexual harassment and violence
To be subjected to unwanted touching, comments or other actions of a sexual nature, with or without violence, is to be subjected to a crime. Being subjected to such actions can also affect one’s health in a negative way. This study presents the results from the Swedish national survey SRHR2017, where a representative sample of the Swedish population was asked a set of questions on, among other things, sexual harassment and sexual assault. The response rate was 31 percent. Despite the survey design and weights, the results should be interpreted with caution. All questions ask about life time experiences. The aim of this report is to describe the Swedish population’s experiences of sexual harassment and sexual violence from a public health and SRHR perspective. The results are presented by sex, age, level of education, sexual identity and transgender experience.
Almost half of all women have been sexually harassed
The results from this survey show that many forms of sexual harassment and sexual assault are widespread in the Swedish population, among both women and men. All forms of sexual harassment, assault and violence are however more common among women than among men, and lesbian, gay, bisexuals and transgender (LGBT) people are more often subjected to these types of assaults, compared to the general population.
The most commonly reported forms of assault were sexual harassment and so-called “other sexual offenses” (e.g. unwanted touching). Four in ten women and one in ten men reported having been subjected to sexual harassment or other sexual offenses. Among women 16-29 years of age, over half reported having been subjected to sexual harassment and a similar proportion reported having been subjected to “other sexual offenses”.
The largest proportion of those who had been subjected to sexual harassment was found among bisexual women, where three out of four reported having been sexually harassed. Gay men were also more often harassed than heterosexual men, with one in three gay men reported having been sexually harassed. The most violent forms of sexual assault, attempt at sexual intercourse through threats or violence and sexual intercourse through physical violence, were most common among lesbians. Gay men were subjected to these types of severe assaults to the same extent as heterosexual women.
The number of people reporting themselves victims of these crimes decreases with age among both sexes.
Results in short:
- Many forms of sexual harassment, sexual assault and sexual violence are common and significantly more common among women than among men.
- Four in ten women in Sweden had been subjected to sexual harassment such as unwanted texts, phone calls, sexual proposals or been subjected to exhibitionists (42 percent among women and 9 percent among men). Over half (57 percent) of women 16-29 years of age and half (48 percent) of women 30-44 years of age has experienced sexual harassment.
- Similarly, almost one in two women and almost one in ten men had experienced other sexual assault such as being forced to touch someone’s body in a sexual way against their will. Over half (55 percent) of women 16-29 years of age and almost half (47 percent) of women 30-44 years have experienced this.
- 11 percent of women and 1 percent of men had been subjected to attempted intercourse by physical violence or threat of physical violence. This also was more common among LGBT-people where 30 percent of lesbian women and 10 percent of gay men had been subjected to this form of assault.
- 7 percent of women and 1 percent of men had been subjected to forced intercourse by physical violence or threat of physical violence.
- 23 percent of women and 5 percent of men had been subjected to sexual assault by psychological pressure. This also was more common among lesbian, gay and bisexual people, 44 percent among bisexual women and 16 percent among gay men.
- 9 percent of women and 3 percent of men had been subjected to sexual humiliation such as for example that someone criticized your body, your sexual desire or capacity, or made you watch porn against your will.
- Homosexual-, bisexual- and transgender people are significantly more likely to report being subjected to sexual harassment, sexual assault and sexual violence than heterosexual and cis-people.
Great need for prevention of sexual harassment and violence
This study shows that many forms of sexual harassment and sexual offenses are prevalent in the Swedish population and mainly affects women but LGBT people are also a vulnerable group.
There is still a great need for preventive measures against sexual harassment and violence. These phenomena are both unacceptable and criminal and must stop. Schools play an important role. Issues such as norms, gender patterns, gender equality, sexuality and relationships need to be included at an early stage in the broad work with knowledge and fundamental values in general, and particularly in sexuality education.
Sex life part A
Sexuality is a significant part of life and it is important for our health and it is closely related to identity, integrity and intimacy. These, in turn, affect our self-esteem, wellbeing, and ability to recover. This study presents results from the Swedish national survey SRHR2017, where a representative sample of the Swedish population, aged 16 to 84, was asked a set of questions on, among other things, experiences and problems in relation to their sex life. The response rate was 31 percent. Despite the survey design and weights, the results should be interpreted with caution. The aim of this report is to describe different aspects of the population’s sex life, such as, sexual satisfaction, how often one have sex and experiences and problems related to their sex life. The results are presented by sex, age and educational level.
The majority were satisfied with their sex life
This study shows that the majority of the Swedish population 16-84 years of age, were satisfied with their sex life, believed that sex is important and have had sex in the past year. The largest proportion of those who were satisfied with their sex life were women aged 30–44 and 45–64 (63 percent) and men aged 30–44 (67 percent). The youngest group among men (16–29 years of age) and the oldest group among women and men (65–84 years of age) were least satisfied with their sex life.
Gender was shown to be of significance for experiences and problems in relation to sex life. For example, it was more common among women than men to have lacked interest in having sex, lacked desire, pleasure and excitement during sex, experienced physical pain as a result of sex and had difficulty in reaching climax. Additionally, more than every tenth woman (13 percent) have had issues with vaginal dryness.
It was more common among men than women not to have had a sex partner, to have reached climax more quickly than they would have liked, not had sex in the way they wanted and to have wanted to have more sex partners. Seventeen percent of men reported that they had trouble getting or keeping an erection.
More women than men experienced that they were too tired or stressed to have sex in the last twelve months. In the age group 30–44, 37 percent of women and 17 percent of men stated that they were too tired or stressed to have sex. Eight percent of the population reported having had health issues or physical problems that had affected their sex life. 13 percent had sought advice or help from the health care system for problems in relation to their sex life, while the majority (82 percent) stated that they did not seek help and did not think they were in need of it.
Results in short:
- 58 percent of the Swedish population aged 16–84 were satisfied with their sex life over the past year and the majority thought that sex is important.
- Four out of five Swedes aged 16-84 (80 percent) had sex in the last twelve months. About every third man or fourth (28 percent) and every fifth woman (18 percent) reported that they had not had sex frequently enough.
- One fifth of women (21 percent) and just under one tenth of men (8 percent) had lacked sexual desire.
- Twice as many women (33 percent) as men (15 percent) had lacked interest in sex.
- One tenth of women (9 percent) and four percent of men had lacked sexual excitement.
- 13 percent of women had issues with vaginal dryness.
- It was more common among women (16 percent) than men (7 percent) to not have reached climax, while more men (18 percent) than women (2 percent) had reached climax more quickly than they wanted to.
- 17 percent of men had trouble getting or keeping an erection. This problem was more common in older men.
- 11 percent of women and 2 percent of men had experienced pain as a result of sex.
- Twice as many women (20 percent) as men (10 percent) had been too tired or stressed to have sex.
- 8 percent have had health issues or physical problems that have affected their sex life.
- 13 percent have sought help for problems in relation to their sex life.
Continued public health work
This study shows that the majority of the Swedish population aged 16 – 84 were satisfied with their sex life during the last twelve months, have had sex in the past year and think that sex is important. The results further show that sex and age affect experiences and problems in relation to sex life. Information, counselling and care related to sexuality should be needs-oriented and should meet the requirements from a public health perspective through: availability, accessibility, acceptability and quality.
Sex life Part B – about sexual identity and transgender experience
Sexuality and sexual identity are important parts of our lives and affect our health and our well-being. Sexual identity is about whom a person has the ability to fall in love with or be attracted to. LGBTQ is an umbrella concept and stands for homosexuals, bisexuals, transgender people and people with queer expressions and identities. This study presents the results from the Swedish national survey SRHR2017, where a representative sample of the Swedish population, age 16 to 84, was asked a set of questions on, among other things, experiences and problems in relation to their sex life. The response rate was 31 percent. Despite the survey design and weights, the results should be interpreted with caution. The aim of this report is to describe different aspects of the population’s sex life, such as, sexual satisfaction, how often one have sex and experiences and problems related to their sex life by sexual orientation and separately for trans people and cis people. The results are presented by sex, age, sexual identity and transgender.
Sexual identity – important to sex life
The majority of heterosexual, gay/lesbian women and men and bisexual women stated that they were satisfied with their sex life. A lower percentage of transgender people said they were satisfied, however, those aged 45 – 64 tended to be more satisfied than other age groups. Bisexual women and men were more often dissatisfied with their sex life than other groups. The results also showed that most LGBT people, as heterosexuals, have had sex in the last year, but that every fourth transgender person and every fifth bisexual man had not had sex.
Sexual identity and sex is of importance for experiences and problems in relation to sex life. Every fifth woman, regardless of sexual identity, had lacked sexual desire and every third woman had lacked interest in having sex. Bisexual women tended to have more difficulty reaching orgasm, wanted more sex partners and more often experienced worry or physical pain as a result of sex than heterosexual women. A larger proportion of lesbian women reported that they were satisfied with their sex life, more often had sex, and had an easier time reaching climax compared to heterosexual women.
Lack of sexual desire was more common among gay and bisexual men (16 percent and 14 percent respectively) compared to heterosexual men (8 percent). In addition, more gay and bisexual men had lacked interest in having sex, had more difficulty reaching orgasm, experienced more worry, and lacked enjoyment and excitement during sex in comparison to heterosexual men. It was more common among gay men (10 percent) than heterosexual men (2 percent) to have felt pain as a result of sex. More than every fifth of transgender person had lacked sexual desire (22 percent), been too tired or stressed to have sex (23 percent) and lacked a sex partner (24 percent). Forty-two percent of transgender people had lacked interest in sex, 26 percent had not had sex in the way they had wanted and 18 percent had health problems or physical problems that affected sex life. In all groups, approximately 15 percent had sought advice or help from the health care system for problems in relation to sex life, while the majority had not sought help and felt that they were not in need of it.
Results in short:
- It was more common among cis people (57 %) than transgender people (34 %) to be satisfied with their sex life.
- 28 percent of bisexual men, 19 percent of gay men and 24 percent of transgender people had not had a sex partner.
- More than every fifth woman, irrespective of sexual identity, had lack of sexual desire.
- 39 percent of lesbian and bisexual women and 32 percent of heterosexual women had lacked interest in sex.
- It was more common that gay and bisexual men had lacked interest in sex (25 percent and 22 percent respectively) as compared to heterosexual men (15 percent).
- 42 percent of transgendered people had lacked interest in sex as compared to 24 percent of cis people.
- More bisexual women (27 percent) had not reached or had difficulty reaching climax compared to heterosexual and lesbian women (15 percent and 14 percent respectively).
- Every fifth gay man (19 percent) had not reached or had taken a long time to reach orgasm, compared to heterosexual and bisexual men (7 percent and 9 percent respectively).
- Every eighth gay man and lesbian woman (10 percent and 12 percent respectively) and every fifth bisexual woman (19 percent) had experienced pain as a result of sex.
- Vaginal dryness tended to be less common among lesbian women (5 percent) as compared to both heterosexual and bisexual women (14 percent).
- Every fifth bisexual man and transgender person (21 percent and 19 percent respectively) had difficulty getting or maintaining an erection.
- More than one in ten lesbian women and gay men (13 percent) and almost every fifth transgender person have had health problems or physical problems that had affected their sex life.
- About 15 percent sought advice or help for problems in relation to their sex life, while the majority had not sought help and considered that they were not in need of it either.
Continued public health work
This study shows that the majority of the Swedish population, regardless of sexual identity, are satisfied with their sex life. A majority have had sex in the past year and thinks that sex is important. The results further show that sex, age and sexual identity affect experiences and problems in relation to sex life and that there are differences within and among different groups. It is important to look at sexual health from a holistic perspective, which includes understanding of the synergies between sexual, physical and mental health. Problems associated with sex life exist among all groups, but some problems might be more common in some groups. Information, counselling and care related to sexuality should be needs-oriented and should meet the requirements from a public health perspective through access, accessibility, acceptability and quality.
Sex, relationships and sexual empowerment
Integrity, voluntariness, and consent are basic prerequisites for good sexual health. Free decision making over ones’ own body is also a human right. The concept of sexual empowerment describes an individual’s perception of autonomy and decision making over when, how, and with whom to have sex. In the survey SRHR2017, a representative sample of the Swedish population aged 16–84 answered questions on sexual and reproductive health and rights. The response rate was 30.5 percent. Despite the survey design and weights, the results should be interpreted with caution. The aim of this report is to describe the results from SRHR2017 regarding sex, relationships and sexual empowerment. Differences in sexual empowerment based on sex, age and level of education
- A majority of the Swedish population think sex is important in a romantic relationship, feel free to take sexual initiatives, can say no to having sex, know how to suggest to a partner how they want to have sex and know how to say no if a sex partner wants to do something they do not want to do. However, this does not apply to all humans. There are some differences based on sex, age and level of education.
- Approximately half of women and men reported that they and their partner equally often decide when and where to have sex. It was more common for men to report that their partner decided where and when to have sex in the age bracket 30 to 64.
- A larger percentage women, as compared to men, most often feel free to take sexual initiatives, know how to say no to having sex, know how to suggest how to have sex and know how to say no if a sex partner want to do something they do not want to do. However, for all these questions a larger percentage of men, as compared to women, responded “Yes, sometimes”.
- Educational attainment and sexual orientation also influences sexual empowerment
- It was more common among men with longer education to state that they decides when and where to have sex, as compared to men with shorter education. On the other hand, it was also more common among men with longer education to state that their partner decides when and where to have sex.
- Men with university education know how to say no to have sex to a higher degree, as compared to men with shorter education.
- Women with university education are more likely to find sex in a romantic relationship to be important, know how to take sexual initiatives, and tend to more often be able to tell a partner how they want to have sex.
- Few differences based on sexual orientation were statistically significant. Bisexual men were less likely to feel free to take sexual initiatives, as compared to heterosexual and gay men.
- Trans people tended to be less likely to say no when a sex partner wants to do something they do not want to do, were less often able to say no to have sex, were less likely to take sexual initiatives, as compared to cis people.
Sexuality and digital arenas
In the survey SRHR2017, a representative sample of the Swedish population answered questions on, among other things, sexuality and digital arenas. The response rate was 31 percent. Despite the survey design and weights, the results should be interpreted with caution. The aim of this chapter is to describe different aspects of how the Swedish population used the internet for sex-related activities. The public health agency presents results based on sex, age, sexual identity and educational level.
The current study, in line with previous research, shows that it is common among women and men of all ages to engage in online activities such as searching for sex-related information, reading erotic material, or finding partners. Almost all such activities were most common among 16–29 year olds and became less common with increasing age. There were few or no differences between the sexes among young people aged 16–29 years, while among older people it was more common among men than women to engage in activities related to sex and sexuality online.
The majority of 16–29 year olds had searched for sex-related information, while approximately 50% had looked for a partner online (not primarily for sex) as well as read erotic material. Other activities were less common among 16–29 year olds. Approximately 20–25% had experience of looking for a sex partner online, meeting a sex partner online, putting up or sending pictures, or sexchatting/having had cybersex online.
Among all older age groups, it was more common among men than women to have searched for sex-related information, to have looked for a partner (not primarily for sex), to have met a sex partner, and to have read erotic material. No differences between the sexes were found regarding having bought sex toys online, having put up or sent pictures, or having sexchatted/had cybersex.
Results in short:
- Having looked for a partner online (not primarily for sex) and having looked for a sex partner was most common among younger people and was less common with increased age. Among all other age groups, it was more common among men than women to have looked for a partner or sex partner online.
- It was more common among younger than older persons to have put up or sent pictures or videos with sexual content online. No differences between sexes were found.
- Having read erotic material was more common among younger persons and was less common with increasing age. No differences based on sex were found among 16–29 year olds. In all other age groups it was more common to have read erotic material online among men than among women.
- Having sexchatted or had cybersex was most common among 16–29 year olds, and about one third had this experience. No differences were found based on sex.
Use of pornography and sexual health
It is more common among men to watch pornography, compared to women. Studies exploring the effects of pornography use have come to different conclusions, although many agree that potential harmful health effects can be found among people who are frequent users, meaning people who watch pornography at least 3 days a week. Frequent use of pornography has for example been found to be associated with wanting to try things one has seen in pornography in real life, sexual risk taking and with attitudes supporting violence against women (ASV).
In the survey SRHR2017, a representative sample of the Swedish population aged 16–84 answered questions on amongst other, experiences and problems related to their sex life. The response rate was 31 percent. Despite the survey design and weights, the results should be interpreted with caution. The aim of this report is to present the population’s responses regarding questions on pornography in SRHR2017 and to present a literature review on pornography.
Results in short:
- Pornography use is more common among men and young people than among women and the elderly, and the differences are considerable.
- 41 percent of male Swedes aged 16–29 and 23 percent of men aged 30–44 use pornography frequently, meaning at least 3 days a week. Frequent use of pornography is uncommon among women, and only 3 percent of women aged 16–29 and 1 percent of women aged 30–44 use pornography on a daily or almost daily basis.
- 48 percent of male and 33 percent of female residents had used pornography in order to increase their sexual experience. This is most common in the age span 30–44.
- Almost half of the consumers said their consumption did not affect their sex life, whereas one third said they did not know if it did affect their sex life or not. A small percentage reported their consumption affected their sex life negatively, 4 percent among women and 4 percent among men. It was more common that men felt their consumption affected their sex life positively (23 percent), as compared to women (14 percent).
- Frequent pornography use was found to be associated with lower self-rated sexual health and with other risk factors such as sex for payment, problematic sexual performance requirements, and dissatisfaction with one’s sex life. There were no differences among frequent users compared to non-frequent users regarding who in a relationship most often makes decisions about how and when to have sex. We cannot make any conclusions about the causation of these associations.
Ways forward for increased equity and equality in health
This is the first time the Swedish Public Health Agency has focused on pornography use and health. The results show that pornography use is a common phenomenon, especially among young men in Sweden. Previous studies have shown pornography use can potentially have a harmful impact on young people’s sex life and the personal sexual script. Women are also negatively affected by men’s pornography use when the pornography is based on an imbalance in power where women always are subordinate which is displayed by violence against women in pornography. En viktig del i det förebyggande arbetet är att diskutera pornografins negativa konsekvenser med pojkar och män, och skolan är en viktig arena för detta. Undervisning om jämställdhet, sexualitet, kön och relationer är också obligatorisk i svensk skola. Det är viktigt att vuxna är öppna för samtal om pornografi, men även för diskussioner kring vikten av respektfulla och ömsesidiga relationer. An important part of the preventive work is to discuss the negative consequences of pornography with boys and men in schools. Gender equality, sexuality, sex, and relationships are compulsory in Swedish schools. It is important that adults have an open mind regarding conversations about pornography, but also for discussions on how to form sound sexuality and the importance of respectful and mutual relationships.
Sex for money or other type of compensation
Transactional sex is used to describe a situation where a person gets, or is offered, compensation or reimbursement in exchange for sex. The compensation can be money, clothes, gifts, alcohol, drugs or a place to sleep. The term is also used when it comes to pay or give other compensation for sex. Since 1999 it is illegal to buy sexual services in Sweden, while selling sex is not. This study presents results from the Swedish national survey SRHR2017 about sexual and reproductive health and rights, including results on transactional sex. The response rate was 31 percent. Despite the survey design and weights, the results should be interpreted with caution. The Public Health Agency presents experiences of transactional sex by sex, age and sexual identity (heterosexual, gay, bisexual and queer [hbq]).
Results in short:
- Having paid or provided other types of compensation for sex was almost only prevalent among men. Nearly one in ten men and 0,5% of women had ever paid for sex
- It was more common among hbq men to ever have paid for sex than among heterosexual men (15% compared to 9%)
- It was more common to have paid for sex abroad than in Sweden, 80 per cent of men who had paid for sex had done it abroad.
- Nearly 5 per cent of men had ever paid for sexual services via internet, mobile phones or applications.
- It was unusual to have received payment or compensation for sex; 1 per cent among men and 1,5 per cent among women. Having received payment for sex was more common in Sweden than abroad among both men and women
- Seven per cent among men and women identifying as hbq had ever received payment or compensation for sex.
- It was uncommon to have sold sexual services on the internet, only 0,5% had this experience. It was somewhat more common among LGBQ-people than among heterosexuals.
Future preventive measures
The group people with experience of receiving payment or compensation for sex is an important target group in the work of the Public Health Agency for sexual and reproductive health and rights, against HIV/STI and for equal rights and opportunities regardless of sexual orientation, gender identity or gender expression.
Since the reasons for having transactional sex and the experiences of the phenomenon transactional sex are very different, the preventive work need to include many different preventive measures from for example public authorities, schools and health care services. The results also shows that experiences of transactional sex are more common among LGBQ-people. People with experience of transactional sex should be offered social support and interventions to improve sexual, physical and mental health, regardless of sex or sexual orientation.
Reproductive health
This chapter presents results from the survey SRHR2017, where a representative sample of the Swedish population answered questions on, among other things, reproductive health. The response rate was 31 percent. Despite the survey design and weights, the results should be interpreted with caution. The aim of the report is to describe the results on contraceptive use, thoughts on wanting or not wanting children, and reproductive experiences such as pregnancy, miscarriage, abortion, and child delivery. The National Public Health Agency presents the above-mentioned experiences by sex, age, educational level, income, and sexual identity.
Results in short:
Contraceptives
- Hormonal contraceptive use is largely due to age, whether one has an on-going relationship, is sexually active, or if one wants to become pregnant.
- Income and educational level, but not cost, affects hormonal contraceptive use among women aged 16–29 . The proportion of women aged 16–29 years using the pill is lower among women with high income as compared to low-income and lower among women with high education as compared to women with low. Other factors that may influence the differences in use include worries about hormones and their side effects but more analysis is needed.
- The withdrawal method (pulling out) and safe periods are used by almost one fifth of women and men aged 16 to 44.
Children
- There is a relationship among both women and men aged 30 and older between socioeconomic position and wanting children as well as with the number of children you want. Men with low education and low income to a lesser extent have the number of children they want.
- Three per cent of women and men aged 30 and above report being involuntarily childless, whereas 5 percent, in all ages, do not want children.
- Approximately 7 percent of both women and men aged 30 to 84 have become parents without wanting to.
Pregnancy
- Approximately one third of Swedish women have had one or more abortions.
- One third have experienced a miscarriage.
Child delivery
- Women aged 30–44 years were 28 years old on average at their first child delivery, whereas women aged 45–64 were 26 years old on average. The longer the education, the older the women were at their first child delivery.
- Twenty-six per cent of women aged 16–84 reported physical difficulties after at least one of their deliveries, 17 percent reported psychological difficulties, and 14% reported sexual difficulties. Experiences of the consequences of child delivery vary with age and educational level. Men also reported psychological and sexual difficulties after attending child delivery.
- Depending on age, 81–92 percent of women who had delivered a child had a vaginal delivery. It was more common among younger than older women to have had a caesarian section. The type of delivery did not vary by income or education.
- Vacuum-assisted, and rarely forceps, delivery was most common among women aged 30–44 (12 percent) years.
- Women having had an episiotomy were most often older than 45 years, while women younger than 45 years had most often had spontaneous laceration that, as the episiotomy had been sutured.
- The majority of women with experience of child delivery had had an episiotomy or a spontaneous laceration, and 8 percent had a rupture without sutures and 4 percent had a rupture involving the anal sphincter (grade 3 or 4).
- Approximately 12 percent had sought care for problems related to episiotomy or spontaneous lacerations in relation to delivery, 7 percent answered that they had received treatment that had helped, 3 percent said that they had not received treatment, and nearly 2 procent said that they had treatment that did not help.
- Age, education level, or income did not affect the seeking or receiving of care or problems related to child delivery.
Conclusions about reproductive health
Hormonal contraceptive use among women in Sweden vary based on age and need but also based on income and education. Thoughts regarding children vary by age and sex but also based on income and educational level. Reproductive experiences such as pregnancy, abortion, miscarriage and child delivery also vary according to a range of factors including age, income, educational level, sexual identity and sometimes geographical region.
Sexuality education – an important part of SRHR
The right to knowledge
All students in the Swedish school system are entitled to evidence based, recurring, relevant and knowledge building sexuality education that forms an important part of the foundation of sexual and reproductive health and rights (SRHR). School is a central health promoting arena and the right to information and knowledge are important parts of the SRHR work in general.
Several national and international guidelines and reports indicate that an evidence based sexuality education creates the foundation for the students to develop their reflective, critical and communicative ability and strengthen the students' opportunities to make informed and responsible decisions in the area of sexuality and relationships.
Few people think that the sexuality education provide enough knowledge
- 19 percent stated that they thought the school's sexuality education had given them the knowledge they needed. More men (22 percent) compared to women (16 percent) stated that the teaching provided them with the knowledge they needed. Almost a third (29 percent) stated that the sexuality education did not give them the knowledge they needed and every fourth respondent (26 percent) acquired the knowledge they needed from a different source.
- 8 percent stated that they never received any sexuality education.
- No significant differences between women and men with different educational attainment were found regarding if one had gotten the sexuality education needed.
- Men are more often satisfied with the sexuality education given, as compared to women and regardless of sexual identity.
- Lesbian/gay (39 percent) and bisexuals (36 percent) more often reported that their sexuality education had been inadequate, as compared to heterosexuals (28 percent).
- In comparison with UngKAB15, there is somewhat fewer in SRHR2017 that thinks that sexuality education has given them sufficient knowledge. In UngKAB15, 58 percent of the boys and 41 percent of the girls, aged 16-29, stated that they received sufficient knowledge through sexuality education. The corresponding figures in SRHR2017 are 37 percent for boys and 26 percent for girls.
Teachers need more competence and governance
The prerequisites for a work of high quality are found in the Swedish curricula. Even so, sexuality education in Sweden has problems regarding equality and quality according to quality reviews carried out.
In order to achieve equality and high quality, teachers' skills and confidence to handle these issues need to increase. Teacher education must address these issues and equip teachers for the work, and for the teachers in service there should be opportunities for competence development.
A prerequisite for this work is the governance from the headmaster or other school leaders and these perspectives must be integrated in the systematic quality work and be planned, monitored and evaluated regularly.